DIABETIC NEUROPATHY AND FEET
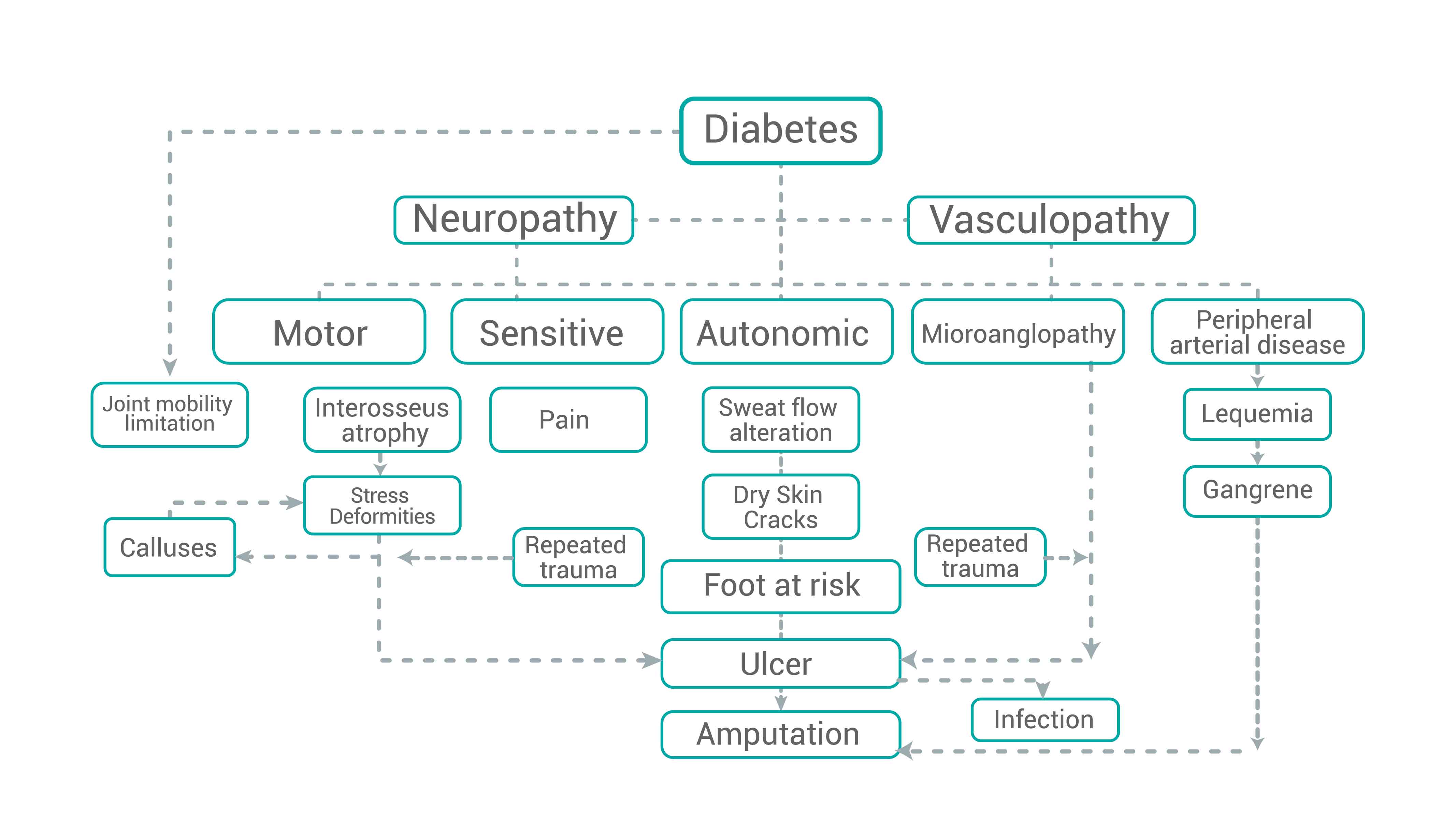
Diabetics are more susceptible to foot problems due to neuropathy and consequently loose or have a decreased sensitivity to pain. All nerves (sensory, motor and autonomic) are susceptible to damage because of diabetes. Diabetic neuropathy syndromes can be divided into acute (self-limited) which present a sudden pain attack or into a weakness that usually resolves itself within 10 months.
Chronic (persistent) diabetic neuropathy is more frequent than acute neuropathy. Symptoms are progressive and include an irreversible loss of sensation. The severity of the symptoms is proportional to the age one’s lived with diabetes. Small diameter fibers (pain, temperature and autonomic information) are affected first; then large diameter fibers (proprioception, fine touch and motor). Vasomotor control is lost leading to tissue hypoperfusion. When normal capillary reflexes are lost, a dependent capillary hypertension and decreased vasodilator response to heat occur. Sympathetic denervation prevents perspiration and the skin becomes dry and brittle, which leads to changes in pH and microflora.
Motor neuropathy comes up at the end, affecting the intrinsic foot muscles with atrophy of the interosseous, causing an imbalance between the extensors and long flexors. This leads to protrusion of the metatarsal heads leading to a hammer-shaped deformity of the fingers. The foot’s biomechanics are altered as the support points are changed, modifying one’s normal walk. Excessive friction on the sole skin causes callosities and continuous pressure leads to ulcerations on the metatarsal heads. Neurogenic ulcers or “poor sole perforator” occur at the first, second and fifth metatarsophalangeal joints. In the soles, the thick calluses can act as a foreign body, causing damage to the soft tissues with capillary blood and serum extravasation, leading it to be a medium for local or external bacteria to grow and produce an abscess, which will help the infection invade the adjacent joint and metatarsal head more easily, causing osteomyelitis. The final part of the sensorimotor disease leads to the so-called Charcot joint (neurogenic arthropathy).
It’s very rare for vasculopathy (peripheral vascular disease and microangiopathy) to be the precipitating event for diabetic foot ulcers; however, they do play a major role in healing the wound and the gangrene development and is a contributing factor for half of all amputations. Although the underlying or triggering event for an ulcer is often trauma, peripheral vascular diseases is the underlying base for the pathophysiology of this diabetic foot complication. Even when the ulcer’s pathogenesis is neuropathy, a vascular etiology for neuropathy has been postulated.
The main factors that contribute to vasculopathy in diabetic patients are: Atherosclerosis, vascular degeneration due to hyperglycemia, increased blood viscosity (endothelial damage), chronic capillary hypertension, hyperinsulinemia atherogenesis, increased coagulation factors, increased platelets aggregation.